You can still watch the Migraine World Summit recap for free! I’m not sure how long the extended version will be available, but it’s right here.
The summit also announced that there is an extended discount if you would like to own the full 2025 library of migraine-fighting information. The discount is available until the 6th of April, and can be accessed right here: Access Passes
Funds raised through the access passes will be used to further cutting-edge migraine research and advocacy.
We’ve talked before about vitamin B12 as a possible migraine-fighter. You may have had your vitamin B12 levels tested, and found in the normal range. But is the “normal range” wrong?
Of course this will very much depend on the lab that does the test, or the country you’re in. A recent study published in the Annals of Neurology (February 2025) turned up problems in people with “acceptable” B12 levels – acceptable, but in the lower range.
Dr. Alexander Mauskop of the New York Headache Center commented on the study:
The current normal levels for vitamin B12 were determined decades ago, and it is not clear how reliable the research that led to these values was. Quest and Labcorp, two major chains of laboratories, define normal levels as 200 – 1,000 pg/ml and 232 -1,245 pg/ml, respectively. The WHO considers 480 pg/ml to be the bottom of the normal range, while it is 500 pg/ml in Japan. Some experts suggest these higher standards may contribute to lower rates of Alzheimer’s and dementia in Japan.
Dementia is only one possible result of low B12 – weakness, anxiety, and even numbness may be symptoms. And of course we’re concerned about headache and migraine, which is related to overall brain health.
It may be wise to have your levels checked, and to ask for the actual number. If you’re “normal” but in the low range, try at the very least to increase the vitamin B12 in your diet, or talk to your doctor about supplements.
Vitamin B12 deficiency is fairly uncommon, but it wouldn’t be surprising if at least 1 in 25 people had a deficiency, and the number may be even higher if the “acceptable” levels are wrong.
Low levels may be caused by diet, or be more common with age. But there are other possible causes, such as certain medications (e.g. metformin and antacid medications) and especially gut/stomach conditions and diseases. Alcohol abuse can also cause problems with B12 absorption.
It’s almost time for the Migraine World Summit! Now that the summit is an established part of the fight against migraine, some people may wonder why we keep coming back.
This brief video is worth showing to your family and friends to give them an idea why the summit is so valuable. Check it out, and share! Remember, you can register for free right here. This year’s summit is the 20th – 27th of March.
… By the way, do you want to learn more about those 10 year impact statistics and where they come from? Click here for more…
Last year the well-known medical journal Headche published a study about migraine in the United States that was disturbing, to say the least. It seems that all the new awareness of migraine hasn’t had the impact that many hoped it would.
First of all, looking back over 30 years, the researchers found that the prevalence of migraine hasn’t changed much. About 13% or so of the population have migraine. In a group of 100, about 73 of those would be women, and 26 would be men.
Now, if you believe that migraine is a difficult-to-treat genetically based disease, you might say, “Sure, the number of people with migraine may not change much. But we’ve learned so much more about how to treat them – so these people now have better treatments, and so fewer and less severe attacks!”
Except, the data isn’t telling us that either.
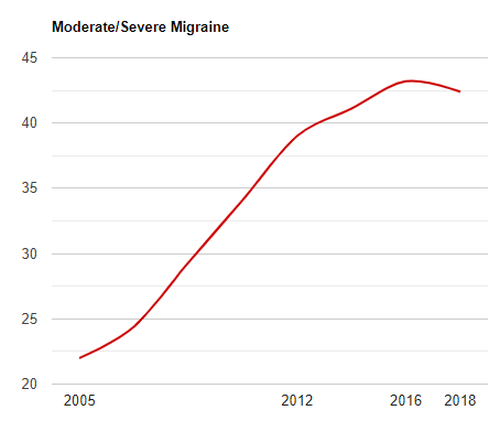
Using the MIDAS test, which measures disability from migraine, the researchers found that the trend is generally toward more disability, not less. This chart gives you an idea how many people with migraine are suffering with moderate/severe disability.
(Note – the study only had data for the years shown, so the graph is a smoothed-out estimate.)
It looks bad – and it is. However, we should note that there are some possible weaknesses in the study. For example, the estimates are only as good as the actual reports we get. Is it possible that more people are taking migraine seriously? More people are seeing their doctors?
Is the (slight) downward trend we see starting in 2018 a sign of things to come?
Maybe. But the results are still disturbing. The fact remains that the percent of migraine patients with significant disability almost doubled between 2005 and the most recent measurement!
Why aren’t we making more progress? Dr. Josh Turknett made some comments in December to consider. You can watch his video for yourself, but here are some points he made:
Preventative medications often either don’t work, or only work temporarily.
Abortive medications are also of limited use, often leading to – more abortive medications, and worse migraine disability.
He also implies (rightly, I think) that lifestyle changes are under-appreciated, to say the least. Many specialists may have better knowledge of migraine medications, and even better medications, but they’re still over-focused on prescribing medications and under-focused on things like diet.
By the way, I would recommend Dr. Turknett’s book to you – The Migraine Miracle. It’s a great place to start if you want to get beyond “the next pill” in your migraine treatment.
I would add some other thoughts about why we’re not doing as well as we could be in migraine treatment.
It could be argued that we have better, more targeted medications for migraine today. Although these medications seem to help some who have not been helped by other treatments, statistically speaking they also help those who might already be helped by another medication. In other words, saying that a certain medication may help 10% of migraine patients is not to say it will help another 10%. If that were the case, migraine would have been virtually eradicated by now.
The hype does not always match the reality. New medications come with new side effects, and they do not help everyone.
The hype can also take the focus away from lifestyle changes. There will always be a “new and better” migraine medication on the horizon. Don’t get me wrong – I think that research should continue, and that these medications may be helpful for certain people at certain times. But lifestyle is an incredibly powerful tool – to ignore it means that migraine will only get worse.
Having been involved in migraine research and advocacy for many years, I have seen many people who have found relief. The trend may be disturbing, but the trend does not have to be you. There is hope, and knowledge is an important step.
So even in the area of new medications and research of future medications, I do see a benefit. However, I agree that if we don’t take a serious look at the incredible healing power of lifestyle changes, the situation will not get better.
Here we are at the end of another year! It’s been a year of the unexpected for me, but maybe every year is like that.
But let’s look back at some of the key posts from the past year that you might have missed. I hope this site has been a help to you, and that it will continue to give you information and tips for better health!
This year I’ll put the posts under certain categories…