Another study came out this year linking high blood pressure (hypertension) with migraine. But not for everyone.
The study, published in July, found the link only in women – however, the researchers noted that the number of men in the study was small, so a larger study may show a risk for men as well.
The link was specifically related to diastolic blood pressure. When your blood pressure is taken, it will have two numbers – a higher number and a lower number. The higher number is more commonly linked to cardiovascular problems, but both numbers are important and both numbers can be “high”. The lower number is the pressure of blood vessels “at rest” – diastolic blood pressure. You can see a typical chart of numbers here.
Essentially, higher diastolic numbers meant a higher chance that that particular woman also suffered from migraine.
The link between migraine and stroke and other cardiovascular problems seems to be well established. But we’re still learning just how to understand the connection. The fact that only the one blood pressure number related to migraine tells us that we may need to look at “non-traditional” numbers when we investigate migraine and heart problems.
Meanwhile, at the very least this study is another link between migraine and hypertension. While you’re looking for effective migraine treatment, it’s also important that you take care of your heart. A healthy lifestyle should help with both headache and heart issues.
The prediction and diagnosis of migraine is changing fast, although in some ways it’s not changing at all.
Since the dawn of time, patients and doctors have been able to predict headache attacks to a certain extent, and to notice what prevents them or triggers them.
But then along came more sophisticated computers. The computer can analyze large amounts of data all at the same time, in a way a human can’t. As long as it’s fed numbers, it can search for patterns. Huge medical studies have shown us new patterns that we never would have noticed as humans, even if we had collected all the information together.
Then along came the ubiquitous smart and surveillance devices. The ease with which we can take certain measurements of ourselves and others means more data for the computers, and so the discovery of new patterns.
So ever since the smartphone came along, developers have been trying to come up with apps that could predict migraine attacks, identify triggers, and even recommend personalized treatments. An early success what N1-Headache, formerly Curelator, which began to question some common beliefs about migraine triggers.
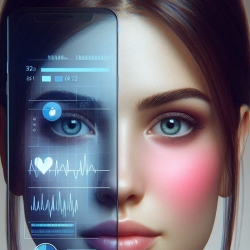
One area of interest that you need to know about is rPPG – that is, (brace yourself), remote photoplethysmography.
So imagine this. You’re on a video chat with someone, and their computer is actively analyzing the video feed. On the other end, information starts popping up on the other person’s screen:
This person is nervous about what you just said.
This person will probably have a migraine attack within the next 24 hours.
This person is at high risk of [a certain disease]
Or perhaps you’re not even on a video chat. Maybe there just happens to be another camera in the room, watching you. Or maybe a computer is going over your social media posts and photos.
Remote photoplethysmography is one method of measuring visible changes in your body, such as in your cardiovascular system.
Now I’ve started out presenting this in a rather negative light. The positives are obvious for you personally, and for the medical community. Gathering huge amounts of data about migraine patients will hopefully lead to some leaps forward in migraine treatments.
Collection of personal data can help you customize your own treatment, and sharing that data – even anonymously – can help you compare your situation to other similar patients. This is much more powerful that an online forum where you meet someone with similar symptoms!
The use of AI to go through the huge amounts of data out there is a developing area of research, as you can see for yourself with a quick search online. Although in many ways it’s not so new, it is becoming much more powerful. How will you use it? How might you try to limit the sharing of your data, or do you care? It’s time to think all this through, because the future is here.
Led by researchers at the University of Oxford, and published in the British Medical Journal, a new study compares migraine medications to find out which is “best”.
Well, they would not phrase it that way. Really, they were trying to judge which medications had the best results in good clinical trials. This is important, because information like this can tell doctors which medication they might want to try with “person X”.
But, of course, there is no “person x”. When a specialist recommends a medication, they should be aware of your medical history, symptoms, and even family history. Study co-author Elena Ruiz de la Torre said it well – “Migraine is a very personal disease”. As also quoted at NewScientist, migraine expert Dr. Peter Goadsby adds that these studies “tell you about a population, but they’re very blunt instruments for trying to understand what’s going on at an individual level.”
With that warning in mind, it is still helpful to have these studies, and here’s what they found.
The now “older” migraine medications, the triptans, are still great tools. In fact, in these studies they are beating out the newer CGRP related medications such as lasmiditan, rimegepant, and ubrogepant.
So the report gave great marks especially to eletriptan, and after that rizatriptan, sumatriptan, and zolmitriptan.Interestingly enough, the humble ibuprofen also got high marks in this report.
In other words, these were the medications that had the best evidence for getting rid of pain and having few side effects.
Again, remember that the newer drugs are helping people that did not respond well to the triptans. And there may be medications and treatments that are better for treating certain people with certain symptoms.
The authors summarize their conclusion based on the studies they reviewed:
Results on both benefits and harms should inform shared clinical decision making, considering the preferences of patients, caregivers, and healthcare professionals. Our findings should help inform future guidelines and updates to recommendations to ensure that patients receive optimal care. Overall, the results of our network meta-analysis suggest that the best performing triptans should be considered the treatment of choice for migraine episodes owing to their capacity for inducing rapid and sustained pain freedom, which is of key importance for people with migraine. While the recent introduction of lasmiditan, rimegepant, and ubrogepant has expanded options for the acute treatment of migraine, the high cost of these newer drugs, along with the substantial adverse effects of lasmiditan, suggest their use as third line options, after the less expensive, similarly efficacious, second line options such as ibuprofen, acetylsalicylic acid, diclofenac potassium, almotriptan, and frovatriptan have been considered.
So the moral of the story? The general guidelines out there don’t seem to be far off, and this is no time to throw out the old just because we have the new. All things equal, if you’re thinking of trying a medication for migraine, talk to your doctor about the triptans. But be sure your doctor knows your situation. You are not “person x”.
Don’t be alarmed. This is not an article about how migraine is making your teeth fall out. Neither is it about how missing teeth causes migraine. This is, however, an article about the relationship of missing teeth to migraine.
Those with migraine know that there are many things that can trigger migraine attacks, make migraine attacks more frequent, or make them worse. A recent study published in The Journal of Prosthetic Dentistry compared missing teeth to migraine pain and found an interesting relationship between the two.
It seems that missing teeth can indeed increase your chances of migraine and severe headaches. Interestingly enough, this was more of a problem with your back (posterior) teeth – think molars – and not so much the teeth in the front. However, a combination of missing teeth in the front and back was also a problem.
As you might guess, more missing teeth also meant more headache pain.
Since this study was in a journal about prosthetic dentistry, you will be glad to hear that there was no problem with teeth that had been replaced.
Why might this be? Well, problems with the mouth and jaw certainly have had a historical connection to migraine. The nerves in your face and neck and how your joints function certainly can cause problems.
The good news is that this is not a huge trigger. For example, one more missing tooth in the back meant a 4% higher chance of migraine or severe headache.
So yes, get that tooth replaced if you can afford it. Your teeth are there for a reason, affecting much more than just your ability to eat celery.
However, don’t expect that prosthetic tooth to cure your headaches. It’s only one more thing you can do improve your life a little bit, and hopefully cut down on the pain over the long term.
A new study is helping us to further understand vestibular migraine (VM) and related types of migraine. The study, published this spring, tried to identify more specifically some of the symptoms that patients with VM experience.
Understanding and identifying these symptoms will help you and your doctor find better treatment. Let’s take a quick look at what the study found:
Ongoing Dizziness?
Officially, vestibular migraine involves temporary symptoms, lasting during part of or all of your migraine attack. However, the study found that many patients experience at least some level of dizziness between attacks. In fact, almost half reported almost constant dizziness. The researchers suggested that this should not lead doctors to write off VM as a diagnosis.
Persistent Postural-Perceptual Dizziness (PPPD)
The researchers define PPPD in this way:
This disorder presents with non-spinning vertigo, dizziness, or unsteadiness occurring on most days for at least 3 months, and worsened by movement, upright posture, and exposure to moving or complex visual stimuli.
It looks like PPPD may often go hand in hand with migraine (about 1/3 of patients with PPPD also have migraine) – especially VM (about 17%). In fact, knowing that VM patients may have symptoms between attacks, the two disorders may “blur” into one another, being confused.
Mal-de-Debarquement Syndrome (MDDS)
Literally “landing sickness” or “disembarkment syndrome”. You know how you get off the boat and you feel like you’re still moving? This goes to extremes in people with MDDS. In fact, some patients just develop it for no known reason, spontaneously. Patients with MDDS do indeed have a higher likelihood of migraine.
Tinnitus
Tinnitus is a perception of noise in the ear, often a “ringing”. 25-50% of VM patients report tinnitus. Tinnitus can be very difficult to treat, but researchers point out that some patients do indeed improve when they treat their migraine attacks.
Other Hearing/Ear Issues
This would include a sense of fullness in the ears, noises in the ears, or actual loss of hearing. Many of these things do seem to be linked to migraine, and again, treating the migraine may also treat the hearing disorder.
Perceptual Symptoms
Once again, we’re putting a whole range of symptoms under one title. This would include things like feeling like things are out of proportion, farther away or closer. It could also be the feeling that time is moving too fast or too slowly. There may even be visual distortions, kinds of hallucinations. There’s a long and fascinating list in the study under this heading.
Many of these symptoms may be a part of a migraine attack, but there could also be another underlying symptom.
Why This is Important
It’s important to know the various common symptoms so that you can notice them in yourself or a loved one. With the pain of migraine, it’s very easy to overlook other symptoms, especially if they seem to persist even when you don’t have a headache.
Noticing these symptoms can help in two ways:
You may have another condition, which will require a unique treatment.
You may benefit from a specific migraine treatment that will help with these specific symptoms.
Doctors should take a look at this study if they have patients with migraine, and especially VM. But patients should be aware as well of the value of recognizing and naming any symptoms that they notice.
The researchers say it this way:
Vestibular migraine is an underdiagnosed disorder. It may present with a wide range of symptoms, but only a few are represented in the diagnostic criteria. Familiarity with the other non-vertiginous symptoms may help clinicians recognize this diagnosis more often, especially when vertigo is not the patient’s main concern. As many of these symptoms may present in migraine more generally as well, knowledge of the broad range of possible presentations should improve patient care. Many patients who could benefit from migraine therapy will be missed if only the most common migraine symptoms are assessed.