This is a less technical and more personal podcast about my own experience at a sleep clinic. I went for a sleep study (technically called a Polysomnography or PSG) and recorded my impressions from before the study until after I had received the results. Hopefully this will be a help to anyone considering having the study done.
For a text summary of what the sleep study is about, try the Mayo Clinic articles: Polysomnography (sleep study), or quick summary at UKHealthCentre with links to UK sleep clinics. Also, a summary from a clinic in Australia specializing in PSGs for children.
What exactly are migraine associated vertigo symptoms? For that matter, what is migraine-associated vertigo (MAV)? Is it a disease? What causes it? How is it treated?
Another term sometimes used is vestibular migraine. But neither MAV or vestibular migraine are considered specific types of migraine (according to The International Classification of Headache Disorders). So it better not to look at migraine associated vertigo symptoms, but at migraine associated vertigo as a symptom of migraine disease.
Dizziness, vertigo, and motion sensitivity are not at all uncommon in migraine. Some people experience one of these during every attack, for others it comes and goes.
Vertigo could actually be a clue into which type of migraine you have, because some "official" types of migraine are associated with vertigo more than others.
Just because you have vertigo doesn’t mean you have basilar type migraine or hemiplegic migraine. These types of migraine are fairly rare, but vertigo is fairly common in migraine patients. It’s estimated that 25-35% of migraineurs experience vertigo. Sometimes vertigo may be the only symptom of a migraine attack (ie no pain).
So it’s important not to be satisfied with MAV as a diagnosis – this is a symptom, and it could be a symptom of various types of migraine. Of course, your vertigo could be a symptom of something else.
Make sure you talk to a doctor or specialist who understands your medical history. Tell your doctor if you’ve had a history of motion-sickness. Also, tell her how long the vertigo lasts. Do you have other migraine symptoms? Are you a smoker? Have you experienced hearing loss? What does the "vertigo" feel like? Do you get dizzy? Does the room feel like it’s spinning? Do you feel like you’re about to pass out? All these things may be important.
Looking for other symptoms aside from vertigo or dizziness may help your doctor make a proper diagnosis and get you the treatment that will help the most.
What is comorbid with migraine, and what does that mean? Comorbidity basically refers to two conditions that tend to go together. That doesn’t mean that one caused the other. In fact, we usually don’t know why they go together.
It could be there’s a common cause, or maybe one could cause the other. It could be something in the environment, or something genetic, or even a coincidence.
But, of course, when we see the same diseases going together over and over, the coincidence hypothesis eventually goes out the window.
What we do know is that the two (or more) things interact. Sometimes there can be a common treatment. Sometimes it means that you can’t take a certain medication, because it may increase your risk of something else.
So it’s important to think about what you may have on top of migraine disease, and it’s important to talk to your doctor about it.
Now there’s a great deal of debate when it comes to migraine comorbidity. Most of these have pretty good research behind them, but sometimes research conflicts and there’s debate about whether a certain thing should be in the list.
But for what it’s worth, here are 15 common diseases, disorders and syndromes that tend to go hand in hand with migraine. That does not mean you will definitely have any of these . . . just that they seem to be more common in migraine patients than the general population. Ones that seem to be more common come first:
Depression
Anxiety
Stroke
Cardiovascular Disease
Hypertension
Epilepsy
Fibromyalgia
Thyroid Disease
Mania/Bipolar Disorder
Panic Attacks
Raynaud’s syndrome
Restless Leg Syndrome
Essential Tremor
Irritable Bowel Syndrome
Chronic Fatigue Syndrome
Now wait – did I miss one that you’re familiar with? Or have you found one or more of the 15 to be true of you? Leave a comment, and let us know how knowing this has helped or hindered in your treatment.
And if you’re thinking about the connection for the first time – talk to your doctor!
In the last post we introduced two concepts – visual snow (VS) and persistent migraine aura (PMA). The first is a specific symptom which can have a number of causes; the second a diagnosis which can include the first.
First, persistent migraine aura (PMA) is diagnosed when other causes are ruled out. But as we’ve said there are a number of things that can cause visual snow (VS).
Doctors will take a careful drug history for patients with VS, because one cause is hallucinogenic drugs. The drug may only have been taken once, and time may have passed since it was taken, but it can have permanent effects.
Optic neuritis, an inflammation of the optic nerve, can also be a cause. Optic neuritis usually develops from an autoimmune disorder. Read more about optic neuritis here.
There are many other things that can be involved – even vitamin deficiencies.
Dr. Klaus Podoll, Dr. Markus Dahlem and Sofia Greene list common tests that are done for persistent aura symptoms here. These include:
Ophthalmologic examination
Neurological examination
Psychiatric examination
Thorough headache history and family history
Thorough drug history (including illegal drugs, especially hallucinogens: LSD, Ecstasy, mushrooms, other?)
CAT or MRI of head (the MRI is important to rule out what is called a migrainous infarction)
Other examinations may follow, including an EEG, evoked potentials (a testing of the functioning of the nervous system), blood work, and a lumbar puncture.
Obviously, if anything shows up on these tests, you’ll be following that up.
Assuming these treatments are out of the way, there are some treatments that have been tried, with some success. There is no tried-and-true established treatment, but some options include:
valproic acid
acetazolamide
lamotrigine (particularly for VS not classified as PMA)
topiramate (Topamax)
Sometimes injections of furosemide (frusemide) are used, if other treatments fail. Clonazepam is also used for patients who have symptoms from hallucinogenic drugs.
Do you have experience with ongoing migraine aura, or visual snow? Have you found anything that has helped? How did the symptoms start?
We’ve talked a lot about migraine aura – especially visual aura – here in the past. Typically, visual aura hits before an attack of pain in migraine, although sometimes it hits all by itself, and can be quite debilitating in its own right.
But what if that visual aura never went away?
That’s what does happen to some people. I’ll get more specific in a moment, but first a couple of important notes…
Is this migraine?
There is some debate over whether these visual symptoms should come under the classification of migraine at all. Now of course, there are many things that can cause aura-like symptoms, shall we say. So of course those other issues need to be ruled out before you can even consider whether or not this is migraine-related.
Next, we have to ask if the visual symptoms are the same as migraine aura, or if they have unique properties. This could mean there is a different cause, though it still could be that there is a root cause involved in the migraine attacks and the visual symptoms.
Finally, even if the symptoms are the same, there is still debate over how closely they are related to migraine. Does the patient have individual migraine attacks? Could there be a common cause of both? Could it be a similar symptom from another cause? These are difficult questions to answer, though we certainly seem to be getting closer to answers as our understanding of the brain increases.
What is Persistent Migraine Aura and Visual Snow?
Last year I was corresponding with someone about persistent migraine aura, and visual snow, and they pointed me to some helpful information. I would give them credit, but for some reason I can’t find the correspondence at the moment (what? James isn’t perfectly organized? I’m so disillusioned!)! But I appreciate the nudge to post on this topic.
Persistent Migraine Aura (PMA), also known as persistent aura without infarction, is diagnosed when there are aura symptoms lasting more than a week without evidence of infarction (which refers to the death of brain cells). This is in a patient that already has migraine with aura, and then has symptoms that are typical of their migraine attacks but lasting longer.
Often these symptoms are only on one side, though not always. They can continue for weeks, even years.
Visual snow (VS) is a more specific symptom, which could be a part of PMA or not, or even a symptom that is a part of a totally different diagnosis.
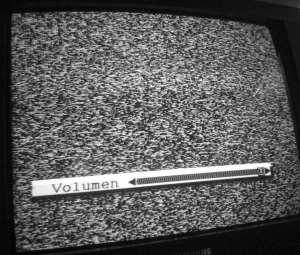
As you might guess from the name, VS is when the person sees "snow", like static on an old TV, all the time. This may be a temporary condition, or pretty much permanent. VS is often accompanied by other symptoms, and other types of visual disturbances, as the video below illustrates:
What’s causing it?
That question doesn’t always have an answer. As mentioned above, often it’s related to migraine and considered a part of migraine disease.
Sometimes there are other causes – at least suspected causes. Research on VS is extremely limited, and though the visual symptoms do have some patterns and relate to other symptoms, it’s sometimes hard to know if there’s a solid related cause, or just two things that are comorbid (that tend to go together, though we may not know why), or if there’s just a coincidental relation.
In our next post on the topic, we’ll talk a little more about possible causes, and what treatments have been suggested.
For now, remember that this is a condition/symptom that is known by (some in) the medical community, and if you’re suffering from it you are by no means alone.