Botox for Migraines: Will it work when other treatments don’t?
Are patients who take Botox for migraines actually improving in the real world? In other words, are their migraine attacks actually decreasing, and is their quality of life improving? And what about patients that don’t respond well to other treatments?
Dr. Modar Khalil at the Hull Royal Infirmary in the UK has been studying headache disorders for a number of years, and most recently the use of Botox (OnabotulinumtoxinA) for migraine. His latest Botox study followed 465 patients treated in England for migraine.
It’s important to note who these patients were. First, they had a median history of four years with chronic migraine. They averaged 15 migraine attack days per month and 27 headache days. And 97% had already tried three or more preventative treatments without success.
So these aren’t people who occasionally get a headache, these are patients whose lives are seriously and constantly affected by migraine.
The best outcome was for 21% of patients, who had at least a 50% reduction in headache days in the first month after treatment, at least a 50% reduction in migraine days, and double the “crystal clear” days with no headache or migraine symptoms.
59% of patients at least hit one of these targets.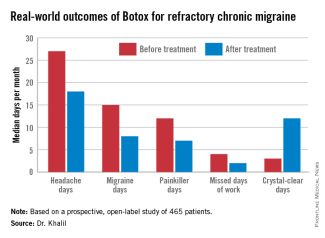
The best results came for those with 21-25 headache days per month – 74% reached at least one goal. Those with more headache days seemed harder to treat (although there was still significant improvement), and those with fewer headache days had less drastic results.
A third of the patients had a 75% reduction in either headache or migraine attack days, and at least three times the “crystal-clear” days.
The medication was tolerated well – the most common problems were a stiff neck (16%) and pain at the injection site (15%) lasting more than 24 hours.
Here are some important things you may want to note about this study. First, these results are very good considering that these are hard-core patients who have had trouble finding treatments that help. At the same time, this was a study of patients in the “real world” – helpful because it shows that Botox actually helps real patients in a normal situation. However, without controls, and without a longer period of time, it is difficult to compare statistically between patients who took Botox and those who tried another treatment, or nothing, or a sham treatment. The numbers would probably be less impressive in a controlled study.
Still, taken along with what we hear in the “real world” about the benefits of Botox (I just received another email from a patient who has been helped significantly by Botox treatment), it should encourage the community to keep pursuing and improving Botox for migraines treatment, and consider its benefits for other chronic headache disorders.
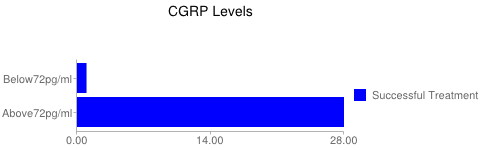
 A study in 2013 showed that women with various types of migraine and cluster had elevated levels of CGRP in their blood (between attacks). Among those with migraine, those with chronic migraine had the highest levels – and among those with chronic migraine, migraine with aura showed the highest levels of all.
A study in 2013 showed that women with various types of migraine and cluster had elevated levels of CGRP in their blood (between attacks). Among those with migraine, those with chronic migraine had the highest levels – and among those with chronic migraine, migraine with aura showed the highest levels of all.