Recently, The Migraine Project ran a successful Kickstarter campaign to raise money for their documentary, “Out of My Head”. Below is the trailer that was used for the campaign. To find out more, there’s another trailer on the Migraine Project page here (be sure to check that one out).
It looks like the film is scheduled to come out by January 2016.
Migraine in children can be very difficult to diagnose. If children have had their symptoms for a long time, it may be normal to them, and you might not even hear a complaint. Or, they will just know they’re “not feeling well” and not be able to explain why.
So, here are 18 reasons to suspect that your child may have migraine. If you suspect migraine, watch your child closely and consider a doctor’s visit.
A close family member has migraine: If so, the child is much more likely to develop migraine than the general population. Do not, however, assume that the child will have the same symptoms or pattern of attacks.
Trips to the bathroom: Vomiting is common in children with migraine. A child may go to the bathroom to throw up and not tell anyone.
Changes in behaviour: Remember, migraine usually isn’t constant. Watch for days when there are changes in your child’s behaviour.
Headache: Migraine attacks in children do not always include headache. But if your child is complaining of headache, it’s not normal. Try to find out as much as you can – how long it lasts, what kind of pain, etc.
“Patterns of avoidance”: Children may not even consciously think about what is bothering them. But a parent may be able to tell if a child is bothered by light or noise. Children also may avoid physical activities that they usually enjoy.
Car sickness: Car sickness may not be migraine, but it may be a sign that the child may develop migraine. Watch for nausea and vomiting when you’re not travelling.
Depression: A child may be depressed because of their symptoms, but depression is also a condition that often goes along with migraine, although scientists aren’t 100% sure why.
Trouble paying attention: Again, remember that a migraine in children will normally last for a day or two at most. Watch for certain days when your child is having trouble concentrating. Ask them how they feel.
Abdominal pain: Often, instead of headache a child will have abdominal pain or discomfort. If you start seeing this come and go, it may be a sign of migraine.
Puberty: Although children do have migraine, it is much more common after puberty hits. In girls, watch for monthly attacks. Do not brush these headaches off as “normal”.
Tiredness: Sleep disorders are common in children with migraine.
Retreat: Children may retreat to their rooms, or go lie down in the dark.
Head trauma: A concussion can lead to certain headache disorders. Be sure to see a doctor and try to avoid further injury.
Trouble at school: Teachers can use these clues as well. But if parents find that their children are having trouble at school, they may discover that migraine symptoms (difficulty in concentrating, avoidance of physical activity, hiding symptoms) may explain some of the problems.
Changes in appearance: Shadows under the eyes, looking flushed or pale.
Hyperactivity: Yes, migraine symptoms may actually cause some hyperactivity. Again, watch for changes in behaviour that last a few hours.
Changes in eating patterns: Avoidance of certain foods, or craving for certain foods.
Headache with Congestion:Congestion, runny nose, watery eyes – all common migraine symptoms.
As you can see, many of these clues could relate to other conditions, or even to just having a bad day. They are not proof of migraine. Also, remember that you may only see one or two of these clues – every child is different, and no child will exhibit all of these.
Watch for something that follows a pattern – you notice certain symptoms on three occasions that go away in a day or two. If you suspect migraine, keep track of the symptoms as much as you can and talk to a doctor.
Photo courtesy of Quinn Dombrowski Her doctor had told her that this day might come – would probably come. But knowing is not the same as being prepared. It’s not the same as knowing what is really coming.
As the symptoms began to show themselves, she wanted to go to the hospital. To take some medication, have some surgery – anything that would alleviate the symptoms or cure her. But she was tired. And she knew that there would be no easy way out.
Why don’t diseases strike at a convenient time? Then again, what would a convenient time be? When I didn’t have that deadline at work? When I wasn’t planning to go out with friends? When I hadn’t planned that precious time with my family?
There’s no reason to think about that now. Even if there was a “good” time, even if I could choose – but I can’t. It’s now. And now always seems like the worst possible time.
I’m still with it enough to call and explain that I won’t be able to make it. No, I’m so tired. I’ll email.
They’re trying to be understanding. “Don’t worry about it!” They’re right – there will be other days. Not this day. But other days. If . . .
But how can they brush it off like it’s nothing? It’s a crisis.
I need help. Who can help? I can’t see. I can’t think.
Time goes by. My body shuts down. Everybody’s body shuts down over time, as they get old – but I’m not old. I’m young. I wish I had a wheelchair. It’s so hard to walk.
There’s a sound coming from outside. What is it? I wish it would stop. I have to get to bed. Where was I going?
Pain! Oh yes, my doctor told me there would be pain. I wish I could take something to stop it. Oh yes, he gave me something – it won’t stop the pain, but maybe it will be a little less.
No. I can’t even take the medication – I’m going to throw up. Was that the phone? Turn it off – someone turn it off!
Pain! So much pain!
When did I go to bed today? I don’t remember. I don’t care. It’s still light. I must make it. I can’t, but I must.
I should have undressed. Who cares? Pain! I wish I had undressed. So uncomfortable.
My mouth is dry. Pain! Why can’t I stop thinking about the pain? Think about something else. Ok – no – regrets – where I would have been in life if I hadn’t – no – can’t think about that – PAIN – can’t think – what is happening?
Need to go to the bathroom. No, I can wait. I can’t get up. Can’t even reach the light switch. If only I could turn over. Wish I had a glass of water. Would I be able to drink it?
There’s that noise outside again – why now? Did I fall asleep? Pain! I’m going to throw up. I know it.
I should call the doctor. But I can’t get to the phone. What was I supposed to do today? What day is it?
I must have slept. Nightmares. Always in every dream the PAIN. Sometimes it’s a person, sometimes an animal, or a fire or a bullet wound . . .
It’s morning. Less pain now. Maybe I can get up. I was supposed to work this afternoon.
Wait – how long has it been? Have I been sick weeks? Months? Why has no one called?
No – now I remember. It was a day and a night. I’m getting a shower. Just a day and a night.
How did I handle so much pain? I didn’t know I could.
I’m showered, dressed. I’m shaking. Still in a cold sweat. I need to eat something.
But I did it. Somehow. I can’t stand up. But I got something to eat. It’s a great victory.
It will take time to recover. A few days. Can I go to work? Should I call in sick?
So silly. Anyone who had lived through that would call in sick for a week. Why wouldn’t I call in sick? Why wouldn’t I tell all my friends – they will be amazed that I survived! Why wouldn’t I?
Most people would enjoy complaining about an experience like this for months – chatting about it in the lunch room while their friends listen with amazement and admiration. Why can’t I?
Because it’s just a migraine. I thought it was a battle with dragons, I thought I survived a medieval battle against incredible odds. I thought a sword had struck me in the head and I just barely made it through, by sheer willpower.
But they say it’s just a migraine. Just a migraine. One of many. Nothing to write about or talk about. Just another one. Is that what it was?
Imagine an old-fashioned but complex machine, based on switches. When you turn on switch A, for example, it supplies power to switches AA, AB, and AC. If you want power to go through these switches, you must turn them on. And so there is a complicated interaction of hundreds of switches.
Don’t worry, that’s about as complicated as this article is going to get. If you grasp the idea of the interaction of switches, that’s enough to understand the analogy.
So what would happen if a switch got stuck? Well, if it were stuck in the “on” position, you wouldn’t be able to stop the power flow through that switch. If it were stuck in the “off” position, neither that switch nor any down the line would ever get power.
This is an over-simplified way to understand the way that some messages are sent through the body. Each cell, for example, relies on something called “ion channels”, proteins which allow a flow of information through the wall of the cell. Imagine it as a switch.
But what would happen if the protein wasn’t properly “programmed”? It might let too much information through, or not enough. It could get “stuck”.
Migraine research is focusing more and more on specific types of ion channels. Consider this statement from a 2011 article in BMC Medicine:
We could now be at a watershed moment in this respect, as the genetic loci associated with typical forms of migraine are being revealed. The genetic discoveries are the latest step in the evolution of our understanding of migraine, which was initially considered a cerebrovascular condition, then a neuroinflammatory process and now primarily a neurogenic disorder. Indeed, the genetic findings, which have revealed ion channels and transporter mutations as causative of migraine, are a powerful argument for the neurogenic basis of migraine.
Many common migraine medications affect ion channels, such as verapamil and topiramate (Topamax).
But researchers are continually looking to new frontiers. And one of these is the investigation into TRPV4, (a nice name for Transient receptor potential cation channel subfamily V member 4). We know that TRPV4 is related to the sending of pain messages in the body. Might it be involved in headache pain?
One of the interesting discoveries that researchers made was the link between TRPV4 and sunburn. When TRPV4 is blocked, so is the sunburn pain (see Could discovery lead to end of sunburn pain?).
Is it possible that the hot pain of many headache conditions could be stopped with the flick of the TRPV4 switch?
Of course, it’s not that easy in real life to find the right switch and turn off pain without causing other problems. And TRPV4 is one of only 30 channels in only on category.
We do know that various factors, such as environment (for example being exposed to chemicals in the air) can turn switches like TRPV4 on and off. In other words, we’re not talking about flipping a switch that was never meant to be switched. It could, for example, be that certain factors, in people with migraine, are flipping switches too often. Perhaps a certain medication could put it back to normal.
This is a huge area of research, but we’re already using medications that involve ion channel “switching”. Better understanding the switches helps us better understand headache and pain disorders, and directs us to the most likely methods of treatment.
If you want to dive even deeper into this topic, check out:
You’ve heard it before. And intuitively, it seems true.
Something starts the migraine chain-reaction. Ok, maybe we’re not sure exactly how that works. But then the blood vessels expand and constrict, the inflammation starts. And as your heart beats and the blood forces its way through your body, it brings on the POUND POUND POUNDING pain of a migraine headache.
But, have you ever really thought about whether that’s actually true?
Throbbing pain is, of course, a typical characteristic of migraine. It’s one of the ways that we recognize migraine as opposed to other types of headache. In fact, in the most recent headache classifications from the International Headache Society, in order to be diagnosed as migraine the pain must have at least two of these characteristics: one-sided pain, pulsating, moderate or severe pain, and aggravated by activity.
But as with so many realities of headache disorders, when researchers actually investigate, they find that the mystery deepens.
For one thing, we have discovered that the constriction and dilation of blood vessels is not always a clear process when it comes to migraine. Advanced imaging studies are discovering that vasodilation, formerly the cornerstone of migraine research, is not a necessary part of migraine after all. (See also this study and Vasodilation and Migraine – The fall of a theory)
Although blood vessels are clearly and necessarily a part of our study of migraine, they may not be related in the way we formerly believed.
And that brings us back to that pulsating pain.
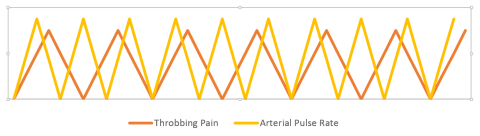
What would happen if we did the obvious, and compared the movement of blood through the body, the heart beat, the pulse, with the throbbing? Well, now we know. It looks something like this…
Notice anything odd? That’s right, the pulse and the pulsating pain don’t match. In this case, the throbbing pain was slower than the pulse. This was typical. But even in patients where the rate of the throbbing and the pulse were similar, they went in and out of sync.
Sometimes the most obvious things about migraine are not so clear once we actually check them out. As you can imagine, the re-thinking of something simple like pulsating pain could have (and is having) huge repercussions when it comes to migraine treatment.
And in this case it’s not just migraine. The same phenomenon has been found in other pain conditions, including other headache related conditions.
Not knowing something can actually be a benefit – as long as you know that you don’t know.
If you want to investigate this fascinating line of research further, check out:


 So, here are 18 reasons to suspect that your child may have migraine. If you suspect migraine, watch your child closely and consider a doctor’s visit.
So, here are 18 reasons to suspect that your child may have migraine. If you suspect migraine, watch your child closely and consider a doctor’s visit.