Hi everyone, I hope you’re having a great weekend! Here are the top posts from the last 3 months – check out the ones that interest you. They are listed with the most popular first, but the posts in bold type had the most likes on Facebook:
The relationship between MS and migraines, and, in fact, MS and headaches in general, is well known. But new research is shedding light on the link between the two.
Multiple sclerosis, commonly known as MS, is a disease of the brain and spinal cord. The National Multiple Sclerosis Society (USA) defines it this way:
Multiple sclerosis (MS) involves an immune-mediated process in which an abnormal response of the body’s immune system is directed against the central nervous system (CNS), which is made up of the brain, spinal cord and optic nerves. The exact antigen — or target that the immune cells are sensitized to attack — remains unknown, which is why MS is considered by many experts to be “immune-mediated” rather than “autoimmune.” Definition of MS
Although it isn’t the norm for those with MS to have a significant increase in headaches, people with MS do seem to be more susceptible. But what kinds of headaches, and why?
According to an article published in the Italian journal Neurological Sciences, the most commonly reported headache types reported by MS patients are migraine without aura and tension-type headaches.
According to a study published this month (Headaches in multiple sclerosis: Cross-sectional study of a multiethnic population.) from the The Keck School of Medicine of the University of Southern California, it’s migraine that is the most common of all. Treatments and socioeconomic status don’t seem to make a difference, but the migraine symptoms are more common among women, especially those who have had MS for a long time.
Migraine is then co-morbid with MS. It’s not necessarily the case that one “causes” the other, but they could also have a common cause or triggers.
However, there is increasing concern that migraine and other headache conditions could actually be an early sign of MS. This would be a rare case, so there’s no need for everyone with migraine to start worrying about MS. But it is yet another reason to see your doctor if you’re experiencing any new headache symptoms.
A report in 2015 highlighted the MS and migraines connection again, suggesting that status migrainosus, a debilitating migraine attack lasting for more than 72 hours, could be an early sign of MS. This report was based on the case of one patient only. But when preventative and abortive medications were not helping, an MRI began the trail of clues that finally led to the multiple sclerosis diagnosis.
Once again, it is important to report any new symptoms to your doctor, whether you’ve been diagnosed with migraine or MS or not. If you are already an MS patient, managing migraine directly and MS directly with current treatments can improve your quality of life significantly.
Although you may need to treat each disease individually, there are times when your doctor may find a treatment that will help with both or avoid a treatment which may worsen symptoms of either MS or migraine.
Whether you’re suffering from a lumbar puncture headache, or you just want to avoid one, this article will help you find the solution. First, let’s take a brief look at why these headaches happen in the first place.
Cerebrospinal fluid (CSP) is a clear liquid that surrounds the brain and spinal cord. It acts in part as a cushion of protection. The body keeps your CSP at a certain pressure.
When this pressure is too high or too low, headaches may warn you of the problem. A number of things might cause the pressure to change, but we won’t get into all of those here.
Courtesy Blausen.com staff. “Blausen gallery 2014“. Wikiversity Journal of MedicineA lumbar puncture, also known as a spinal tap, is often performed in order to get a sample of the cerebrospinal fluid or measure pressure. A needle is inserted into the lower back, between two vertebrae, and the fluid is removed. The same can be used to help diagnose serious infections, cancers and other conditions.
Your doctor may also perform a lumbar puncture in order to inject medicine.
The lumbar puncture itself shouldn’t lead to a significant headache. The problem comes when there is leakage of the CSP after the procedure, leading to an unexpected drop in pressure. The headache that often results is known as a post-dural puncture headache (and in the past has also been called a post-lumbar puncture headache or just lumbar puncture headache).
Incidentally, even an epidural anesthesia can lead to this type of headache. It shouldn’t, but at times the membrane containing the CSP is punctured unintentionally.
Risks, and Avoiding the Lumbar Puncture Headache
The headache is more common in women between 31 and 50 years (older sources indicate a higher risk for young adults – check your sources for more information), and the risk increases if they’ve had the post-dural puncture headache in the past. A small body mass also increases your risk.
The best thing to do to lower your risk is to see a doctor who has experience doing the procedure. Details such as the way the procedure is done and the type of needle used may affect the outcome. Feel free to ask your doctor about these things.
When the Headache Comes
To be diagnosed with a post-dural puncture headache, your headache symptoms must begin within 5 days of the procedure.
One clue to the source of this headache may be that it gets worse when you sit or stand, but gets better when you lie down. This is only a clue – but it isn’t always the case. If that is your experience, it will help your doctor to rule out other possible causes.
It is possible that a headache will start more than 5 days after the lumbar puncture, but you may not get the same diagnosis in that case. There are several related headache types that are very similar.
These headaches may last for a few days, or continue for weeks.
Symptoms often include a stiff neck and even some trouble hearing.
Treatment
For some immediate relief, try lying on your back. If the case isn’t too severe, your doctor may recommend over the counter medication to help with the pain. Most of these headaches should go away without the need of any further treatment.
If you’ve had three days of pain and it’s still going strong, your doctor will probably recommend further treatment. However, do tell your doctor right away if you have a new headache – depending on your situation, some treatments are recommended to be done within the first 24 hours.
A clever procedure known as an epidural blood patch is quite common. A small amount of your blood will be injected to seal the leak with a a blood clot. The pressure should soon be restored, and your headache symptoms will go away.
There are several other treatments that may be tried, whether to quickly seal the leak or to diminish the lumbar puncture headache pain while the problem resolves on its own. If the normal treatments do not work, surgery may be required.
Final notes
Again, the lumbar puncture headache (officially known as a post-dural puncture headache) is only one of the headaches caused by low CSP pressure. The timing of the headaches and the studies your doctor may call for may vary, but the overall idea is similar.
If you’re prone to these headaches, it may be something you need to plan for for the few days after your procedure. However, if possible you should talk to your doctor before the procedure is done about the risks, and see your doctor right away if any headache symptoms develop. If you live with a headache like this for too long, it could end up being a very serious or even fatal condition.
But for most people who are under a doctor’s care, the condition is temporary and will not require any risky treatments.
A new podcast discussing some key articles from past years here at Headache and Migraine News that you might want to check out. A wide variety of topics – brace yourself! 🙂
A new delivery system for migraine medication was just approved in the USA, and it’s been largely flying under the radar. Maybe that’s because people aren’t sure why they would need – or want – to shoot powder up their nose.
Actually, you’re going to want to take a closer look at this medication, so let me take a moment to explain.
Choosing a Medication
Some people have been helped, others not so much, by triptan class medications. But for abortive medications, triptans remain one of the best options in general for migraine.
But some people can take a triptan and find it doesn’t work – then take a different triptan and find that it does work. Perhaps more surprising, they can take a medication in one way with no success, but then take the exact same medication another way and find that it works.
And so researchers often start with a tried and true triptan medication – sumatriptan (a familiar brand is Imitrex) – and try to find a better delivery method to get it to stop the pain, and to stop it as soon as possible.
So there are a lot of options for sumatriptan – tablets, injections, nasal sprays … even a skin patch.
Pros and Cons of Nasal Sprays
Nasal sprays have some advantages. No needle, and no swallowing, for one. But maybe the most key advantage is that they get the medication into your system fast. This is important because – well, you know you want to end the pain as soon as possible. It also tends to be the case that stopping an attack early is easier than stopping an attack later.
But nasal sprays aren’t perfect. Here’s the problem – first, they may be easy to use, but they aren’t foolproof. It is easy to – not spray it quite right (see The Top 12 Mistakes People Make With Nasal Sprays).
Even with an expert sprayer, liquid can leak out and you won’t get the full effect of the medication.
So – Why Powder?
Finally, after all that explanation, we get to spraying powder up the nose. Why would I want that?
Here’s the advantage with powder – instead of leaking and spraying all over the place, it immediately sticks to the inside of your nose and gets absorbed (think throwing flour onto a wet sponge). That means less waste, less room for error, and an extremely fast-acting medication.
Now the developers of Onzetra Xsail have actually done something pretty clever as far as use goes. You don’t technically push a button to spray something up your nose. The problem with that is, you never know if you should exhale, inhale, hold your breath… Instead, you actually blow into the device. This automatically pushes the powder where it needs to go, and you’re done. 2-3 seconds.
This is the “Xsail Breath Powered Delivery Device” (now you get it, right? Xsail?), and it seems to be a great idea, and it seems to be working well for the patients who have tried it. It would be great to see similar innovations for other migraine medications.
Now that Onzetra Xsail has been approved, we begin the process of getting it out to patients, and of course there are other countries which will need to approve it. This could take a while, but the process is in motion.


 The relationship between MS and migraines, and, in fact, MS and headaches in general, is well known. But new research is shedding light on the link between the two.
The relationship between MS and migraines, and, in fact, MS and headaches in general, is well known. But new research is shedding light on the link between the two.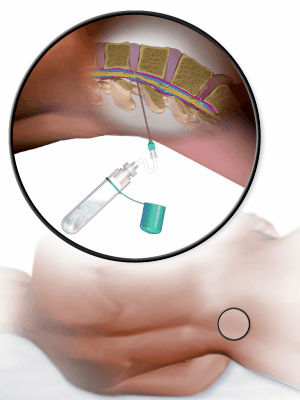

 Finally, after all that explanation, we get to spraying powder up the nose. Why would I want that?
Finally, after all that explanation, we get to spraying powder up the nose. Why would I want that? Now the developers of Onzetra Xsail have actually done something pretty clever as far as use goes. You don’t technically push a button to spray something up your nose. The problem with that is, you never know if you should exhale, inhale, hold your breath… Instead, you actually blow into the device. This automatically pushes the powder where it needs to go, and you’re done. 2-3 seconds.
Now the developers of Onzetra Xsail have actually done something pretty clever as far as use goes. You don’t technically push a button to spray something up your nose. The problem with that is, you never know if you should exhale, inhale, hold your breath… Instead, you actually blow into the device. This automatically pushes the powder where it needs to go, and you’re done. 2-3 seconds.