The onset of silent migraine symptoms can cause a lot of worry, even if the symptoms themselves aren’t too debilitating – which they can be. But are these symptoms something to worry about, or can they be safely ignored?
Migraine aura illustrated by Kathryn GreenhillMigraine aura is not just one thing. Many people are familiar with visual auras, which may include seeing flashing lights, zig zags or patterns. Visual auras can even include a partial loss of vision – either an area of reduced vision or even temporary blindness.
But silent migraine symptoms are not limited to visual auras. An increased sense of smell, trouble speaking or finding the right word, even hearing things – there are a variety of possible symptoms.
The important thing to remember is that these symptoms are temporary, increasing for a few minutes and then typically lasting an hour or less.
Once commonly known as silent migraine symptoms, the condition is now considered a type of migraine called typical aura without headache. It is possible in this type of attack to have more than one symptom, but there is no muscle weakness, fainting or dizziness (if there is, it may still be migraine, but it’s a different type of migraine. For example migraine with brainstem aura).
The symptoms may be an inconvenience, or they can be extremely disabling. Either way, they can be scary because they can look a lot like stroke and other diseases.
If your symptoms are new, or there is a change in symptoms, it is critical to see your doctor right away. When the aura is very short, or very long, or includes blindness over half of your field of vision, your doctor will be particularly concerned and will need to rule out other causes.
Getting Rid of Silent Migraine Symptoms
As strange as the condition may seem, it is not uncommon. And it is a type of migraine. Depending on how disabling the symptoms are, your doctor will discuss with you the risks and benefits of treatments.
As a type of migraine, typical aura without headache is generally treated the way other types of migraine disease are treated. There are many drug and non-drug treatments available – for an introduction, see How to treat a migraine.
Should you be worried? If these symptoms are new or have changed, yes, you should be concerned. If ongoing, your doctor can help you manage them or even eliminate them with proper migraine treatment.
Patients who have tinnitus hear something that’s not from an external source. It can be a ringing in the ears, a whooshing or roaring sound, or even a sort of beating or clicking sound.
Some types of migraine can lead to tinnitus, such as migraine with brainstem aura and vestibular migraine.
There are medications used for migraine which also may lead to tinnitus, such as propranolol or even aspirin. Marijuana and alcohol may also cause tinnitus.
But what is it like to have tinnitus? Can you imagine never enjoying silence – always having another sound in the background, taking your attention away from what’s going on?
But what does tinnitus actually sound like? Well, the The National Institute for Health Research has gathered some examples from the British Tinnitus Association that you can listen to online. Just set your speakers to a normal listening level, and press “play” on any of the 11 sounds.
If you’re like me, you’ll be amazed. And you’ll have more empathy for those dealing with this symptom.
Heartburn medications, such as esomeprazole (Nexium and other brand names), are so common, it’s not surprising that they get blamed for quite a number of symptoms. But some recent studies are making headache patients wonder – is the stomach cure making my head worse?
Esomeprazole belongs to a class of medications known as proton-pump inhibitors (PPIs). Other medications in this class include omeprazole (e.g. Prilosec, Losec), lansoprazole (e.g. Prevacid), and rabeprazole (e.g. AcipHex), among many others.
Headache is actually a common, well-known side effect of PPIs. Other side effects include diarrhea, nausea, and abdominal pain.
If taken for more than three months, PPIs can also lead to low magnesium levels. Migraine sufferers in particular are familiar with the connection between magnesium and their condition. Low magnesium can also lead to general muscle stiffness.
In 2013, a study out of the USA showed that PPI use was related to B12 deficiency. B12 deficiency has been linked not only to cases of migraine, but also dementia. Interestingly, the risk of deficiency was especially high in young adults.
It seems that the PPIs interfere with the absorption of the vitamin.
Last month a study in Germany linked the use of PPIs with dementia yet again.
This does not mean that patients taking PPIs will automatically get dementia, or will automatically have B12 deficiency. And certainly there are people who benefit from at least short term use of PPIs.
However, the risks exist, especially for long term users. With concerns about risk of bone fractures, muscle stiffness, headache and dementia, it might be time to look into other options.
Writing about the recent studies, Dr. Alexander Mauskop of the New York Headache Clinic expressed concerns that tests for B12 levels are often not accurate, and that many doctors will be satisfied with lower vitamin D levels (also associated with dementia) than they should be.
Quitting PPIs
Getting off the PPI treadmill can be a challenge (talk to your doctor), but many patients have done it. The problem is that there can be rebound symptoms after a few days.
Dr. Mauskop’s recommendation – switch to a histamine-2 blocker (such as ranitidine or famotidine (Zantac and Pepcid) and an antacid such as Tums. Watch your diet, and after a few weeks you can stop taking the Zantac and rely only on atacids. Eventually you may be able to avoid the antacids as well.
Another suggestion is to start lowering your dosage of PPIs, for example going to one every day, to one every two days, and so on. Again, you can rely on antacids to get over the hump.
There are many other tips out there – probiotics, for one. Of course a healthy diet is key. But every patient is different.
The relationship between MS and migraines, and, in fact, MS and headaches in general, is well known. But new research is shedding light on the link between the two.
Multiple sclerosis, commonly known as MS, is a disease of the brain and spinal cord. The National Multiple Sclerosis Society (USA) defines it this way:
Multiple sclerosis (MS) involves an immune-mediated process in which an abnormal response of the body’s immune system is directed against the central nervous system (CNS), which is made up of the brain, spinal cord and optic nerves. The exact antigen — or target that the immune cells are sensitized to attack — remains unknown, which is why MS is considered by many experts to be “immune-mediated” rather than “autoimmune.” Definition of MS
Although it isn’t the norm for those with MS to have a significant increase in headaches, people with MS do seem to be more susceptible. But what kinds of headaches, and why?
According to an article published in the Italian journal Neurological Sciences, the most commonly reported headache types reported by MS patients are migraine without aura and tension-type headaches.
According to a study published this month (Headaches in multiple sclerosis: Cross-sectional study of a multiethnic population.) from the The Keck School of Medicine of the University of Southern California, it’s migraine that is the most common of all. Treatments and socioeconomic status don’t seem to make a difference, but the migraine symptoms are more common among women, especially those who have had MS for a long time.
Migraine is then co-morbid with MS. It’s not necessarily the case that one “causes” the other, but they could also have a common cause or triggers.
However, there is increasing concern that migraine and other headache conditions could actually be an early sign of MS. This would be a rare case, so there’s no need for everyone with migraine to start worrying about MS. But it is yet another reason to see your doctor if you’re experiencing any new headache symptoms.
A report in 2015 highlighted the MS and migraines connection again, suggesting that status migrainosus, a debilitating migraine attack lasting for more than 72 hours, could be an early sign of MS. This report was based on the case of one patient only. But when preventative and abortive medications were not helping, an MRI began the trail of clues that finally led to the multiple sclerosis diagnosis.
Once again, it is important to report any new symptoms to your doctor, whether you’ve been diagnosed with migraine or MS or not. If you are already an MS patient, managing migraine directly and MS directly with current treatments can improve your quality of life significantly.
Although you may need to treat each disease individually, there are times when your doctor may find a treatment that will help with both or avoid a treatment which may worsen symptoms of either MS or migraine.
Whether you’re suffering from a lumbar puncture headache, or you just want to avoid one, this article will help you find the solution. First, let’s take a brief look at why these headaches happen in the first place.
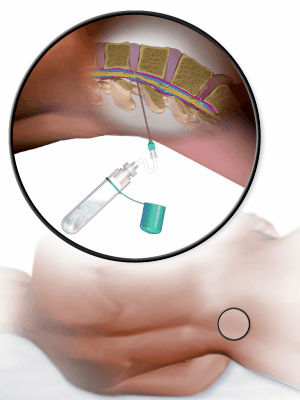
Cerebrospinal fluid (CSP) is a clear liquid that surrounds the brain and spinal cord. It acts in part as a cushion of protection. The body keeps your CSP at a certain pressure.
When this pressure is too high or too low, headaches may warn you of the problem. A number of things might cause the pressure to change, but we won’t get into all of those here.
Courtesy Blausen.com staff. “Blausen gallery 2014“. Wikiversity Journal of MedicineA lumbar puncture, also known as a spinal tap, is often performed in order to get a sample of the cerebrospinal fluid or measure pressure. A needle is inserted into the lower back, between two vertebrae, and the fluid is removed. The same can be used to help diagnose serious infections, cancers and other conditions.
Your doctor may also perform a lumbar puncture in order to inject medicine.
The lumbar puncture itself shouldn’t lead to a significant headache. The problem comes when there is leakage of the CSP after the procedure, leading to an unexpected drop in pressure. The headache that often results is known as a post-dural puncture headache (and in the past has also been called a post-lumbar puncture headache or just lumbar puncture headache).
Incidentally, even an epidural anesthesia can lead to this type of headache. It shouldn’t, but at times the membrane containing the CSP is punctured unintentionally.
Risks, and Avoiding the Lumbar Puncture Headache
The headache is more common in women between 31 and 50 years (older sources indicate a higher risk for young adults – check your sources for more information), and the risk increases if they’ve had the post-dural puncture headache in the past. A small body mass also increases your risk.
The best thing to do to lower your risk is to see a doctor who has experience doing the procedure. Details such as the way the procedure is done and the type of needle used may affect the outcome. Feel free to ask your doctor about these things.
When the Headache Comes
To be diagnosed with a post-dural puncture headache, your headache symptoms must begin within 5 days of the procedure.
One clue to the source of this headache may be that it gets worse when you sit or stand, but gets better when you lie down. This is only a clue – but it isn’t always the case. If that is your experience, it will help your doctor to rule out other possible causes.
It is possible that a headache will start more than 5 days after the lumbar puncture, but you may not get the same diagnosis in that case. There are several related headache types that are very similar.
These headaches may last for a few days, or continue for weeks.
Symptoms often include a stiff neck and even some trouble hearing.
Treatment
For some immediate relief, try lying on your back. If the case isn’t too severe, your doctor may recommend over the counter medication to help with the pain. Most of these headaches should go away without the need of any further treatment.
If you’ve had three days of pain and it’s still going strong, your doctor will probably recommend further treatment. However, do tell your doctor right away if you have a new headache – depending on your situation, some treatments are recommended to be done within the first 24 hours.
A clever procedure known as an epidural blood patch is quite common. A small amount of your blood will be injected to seal the leak with a a blood clot. The pressure should soon be restored, and your headache symptoms will go away.
There are several other treatments that may be tried, whether to quickly seal the leak or to diminish the lumbar puncture headache pain while the problem resolves on its own. If the normal treatments do not work, surgery may be required.
Final notes
Again, the lumbar puncture headache (officially known as a post-dural puncture headache) is only one of the headaches caused by low CSP pressure. The timing of the headaches and the studies your doctor may call for may vary, but the overall idea is similar.
If you’re prone to these headaches, it may be something you need to plan for for the few days after your procedure. However, if possible you should talk to your doctor before the procedure is done about the risks, and see your doctor right away if any headache symptoms develop. If you live with a headache like this for too long, it could end up being a very serious or even fatal condition.
But for most people who are under a doctor’s care, the condition is temporary and will not require any risky treatments.


 Headache is actually a common, well-known side effect of PPIs. Other side effects include diarrhea, nausea, and abdominal pain.
Headache is actually a common, well-known side effect of PPIs. Other side effects include diarrhea, nausea, and abdominal pain. The relationship between MS and migraines, and, in fact, MS and headaches in general, is well known. But new research is shedding light on the link between the two.
The relationship between MS and migraines, and, in fact, MS and headaches in general, is well known. But new research is shedding light on the link between the two.