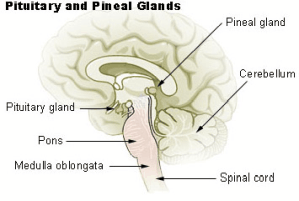
Empty sella syndrome (ESS), or empty sella turcica, is a rare condition in which the sella turcica, a depression in the skull, is partially or completely filled with cerebrospinal fluid, resulting in a displacement or flattening of the pituitary gland. The common name is a strange one, since the sella is not actually empty, which is why it’s also called intrasellar arachnoidocele. But you can see why many prefer the simpler empty sella syndrome, or ESS.
ESS may have a known cause, making it “secondary”. It could be a trauma to the head, a tumour, infection, radiation therapy, or some types of surgery. It could also be “primary”, with no apparent cause.
ESS is rare, and usually goes unnoticed, with no noticeable symptoms at all. But in some cases there are symptoms including – you guessed it – chronic headaches.
There are more likely to be symptoms with secondary ESS, because there are other issues that may cause a problem. But primary ESS is hard to catch. It’s usually found when your doctor isn’t looking for it, through a CT or MRI. Your doctor may also do a lumbar puncture or retinal exam to check for pressure.
Even when it comes to chronic headaches, it is questioned how often the headaches are a result of the ESS, or how often they’re simply coincidental.
When ESS is severe, it could cause high blood pressure, and high fluid pressure in the head. The fluid may even leak out through the nose. The cranial pressure could cause vision problems, even partial blindness.
ESS could actually affect the functioning of the pituitary gland, and lead to symptoms such as decreased sex drive, fatigue, and difficulty staying warm.
If these severe symptoms are present, it may tip your doctor off. But if you just have chronic headaches, it’s likely few doctors would look for ESS specifically, because it’s so rare. However, some symptoms may lead them to check for cranial pressure. For example, you may find your headaches decrease when you’re lying down.
ESS is also more common in obese middle-aged people, and slightly more common in females.
Since ESS is so often symptom-free, even if you have it your headaches may not be connected. You’re most likely to need treatment for the headaches, and not specific treatment of ESS.
There have been some studies into surgery for ESS, in severe cases, and the surgery has helped some people.
No, narcolepsy is not a type of epilepsy that comes from narcotics. In fact, it is neither a disease related to narcotic use, nor a form of epilepsy. Narco in this case comes from a latinized form of the Greek word for stupor or numbness. And yes, someone with narcolepsy is a narcoleptic.
Narcolepsy is actually quite a serious chronic sleep disorder. Basically, sleep can sneak up and attack you during the day – for example, you may be extremely drowsy during the day, you may end up with muscle weakness/slurred speech/loss of muscle control, and you may even experience hallucinations.
Narcolepsy is related to other sleep disorders, so patients may have two or three disorders together.
As a result of sleep problems, many with narcolepsy also gain weight, and have sexual issues (such as a low sex drive, or even extreme sleepiness during sex.
We’re not sure how narcolepsy is related to migraine (although we’ve seen the link before), but a new study seems to show a strong link. Of course, migraine and sleep problems often go together. And fatigue and other symptoms of narcolepsy often accompany migraine, though usually in a different form.
It’s important to try to get to the root of the problem in children. Migraine, narcolepsy, and depression can all be related. And sometimes treating one can help with the other.
Read more a summary of narcolepsy from the Mayo Clinic. If you think that you may suffer from narcolepsy and migraine, this personal story may help you – Narcolepsy and Chronic Migraine. We would love to hear your comments if you’ve struggled with this chronic disorder.
It’s time for an update on our discussion of pillows for migraines. You may remember, this was the topic of a podcast six years ago – The Practical Pillow Podcast. Since then, there has been a lot more written on the topic.
Unfortunately, if you’re simply looking for the “best pillow for migraine” you’re going to be disappointed. Yes, there is a lot of advice out there. But a pillow is a very personal thing. And a pillow that works for your friend may not work for you. You don’t sleep the same way, your headache condition may be different, even simple things like room temperature, or your weight, could make a difference.
So here are some of the most popular pillows for migraines today, and some quick facts about them.
Memory Foam Pillows: Let’s start with the simple memory foam pillow. These have gained in popularity over the past few year, and have helped a lot of people. There are variations on the memory foam pillow, which we’ll see below.
If you haven’t looked at pillows for a few years, you’ll see that things have changed. The technology has improved quite a bit, and there is much more variety. One of the most popular today is the Z Zoned Memory Foam Pillow, which is supposed to be a lot softer than similar pillows from past years. They also make a travel pillow.
A common complaint of these pillows is that they tend to have a manufacture-chemical smell at first. The smell does fade, but migraine patients find they need to leave the pillow out for a while before using it.
Still, many migraine patients used them. One reviewer writes:
I suffer with regular migraines and I quickly learned that the pillow I slept with was a huge factor on whether or not I was going to wake up with a migraine or not so I am very picky, so lets say, used to suffer with regular migraines! Basically I need my head to feel it is floating on a cloud of nothing or I will be miserable when I wake up. I chose the high loft so my head doesn’t “bottom out” and kinda just suspends in this middle of cloudy softness… call me weird in the comments if you want but once you try an amazing high loft pillow you’ll understand what I mean 🙂 [source]
Countoured Neck Support Pillows: Many looking for pillows for migraines immediately think of contoured pillows. Many of these are memory foam as well (which is why I spent extra time talking about memory foam above). A typical example is the inexpensive MEJOY Memory Foam Pillow. If you’re looking to avoid memory foam, check out the Snuz Neck Support Pillow (there is an extra-firm option).
Buckwheat Pillows: Buckwheat pillows have a number of advantages. They provide premium support, being very firm. They have no chemical-smell. They adjust to the shape of your head. And they’re cool. You can even put them in the freezer for an hour before you use them to really cool your throbbing head.
I’ve often talked about buckwheat pillows for migraines. If there is a downside, it’s that they are very firm. It really depends on how you sleep. Also, if you move around a lot, you can hear the shifting of the buckwheat hulls.
“Cooling” Pillows: Because of the pulsing, hot headaches that many of us get, “cooling” pillows are a great option. Now, just a caveat here. Cooling does not necessarily mean that the pillow continually cools you all night. That may be the case if there is constant water flow. But generally it means it doesn’t hold heat in like many traditional pillows do.
One well-known brand is Chillow, but Chillow has changed. Generally what you get today is a “cooling pad” which you can use by itself or with a pillow underneath. You actually put water in the pad. Although some people swear by them, the hassle of adding water and possible leaks have hurt the popularity of Chillow (on the other hand, the price is right if you want to try it!).
A popular and inexpensive example of today’s cooling pillows is the Bluewave Bedding Gel-Infused Memory Foam Pillow. It’s ventilated, and gel-infused, to keep the temperature from rising while you sleep. You can also get very slim versions.
You can also get a pad to put on your favourite pillow, like the Penguin Cooling Pillow Mat. But before you just get a pad, remember you should be changing your pillow every year or two.
As you have probably guessed, there are also combinations of the above. Take for example the ViscoSoft ARCTIC GEL CONTOUR Pillow, which is a hypoallergenic, memory foam, contoured neck pillow!
Changing your pillow can make a huge difference in your health. Many people have found pillows for migraines – that is, pillows that fight migraine, as you’ll see in the reviews for the products above. But sleep remains very personal. You’ll have to try the pillow for yourself to see which one works best.
Final advice? Keep your head cool. If you buy memory foam, be prepared to leave it out of the box for a week or two before you use it. And make sure you make a good pillow a priority. You’ll be spending a lot of time on it!
As we continue to wait for the first CGRP inhibitors to hit the market, clinical trials are giving us more clues about how the medications will actually work.
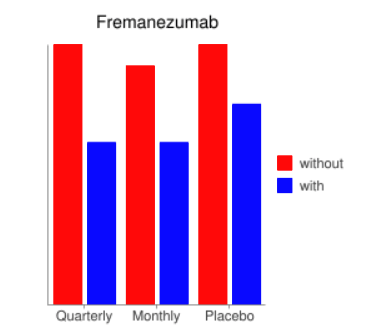
One of the most interesting trials was published at the end of November. Fremanezumab was the drug, and the target group was patients with chronic migraine (that is, headache pain more than 15 days per month, and specifically migraine attacks at least 8 days).
One group received 675mg every three months by injection. Another group had a 675mg injection the first month, then 225mg the next two months.
Now, let’s look at the results.
This is a helpful chart, but let me explain it. There are three sets of data. First, those who had a quarterly injection (before, and after, basically), then those who had a monthly injection, and then a placebo.
So you’ll see that the quarterly and monthly injections were very similar, with the monthly being slightly better. Essentially, about four and a half headache days disappeared on average, or about a third.
Now we know that every patient is different, so here’s some other interesting information. Almost 40% of patients had a 50% reduction in headache days.
I don’t know if you noticed the same thing that I noticed or not, but here it is. The quarterly group and monthly group were very similar. So – for many patients, a quarterly injection may make a huge difference in their lives.
I realize some people hate injections, but for a lot of people, an injection every three months will be a lot better than a pill twice a day.
Obviously with a brand new medication we’re still learning about which doses work best. So hopefully we can find ways to use CGRP inhibitors which will show an even greater improvement for many chronic migraine patients.
Some people have strange ideas about – well, people. Human beings.
Some people seem to think that we’re just MINDS. And since we’re just MINDS, if we think we have no pain, we have no pain.
Other people believe that we are merely SOULS. Perhaps, then, the pain is not even real.
And other people think we’re just BODIES walking around. If we have pain, we have pain. It’s just the way our BODIES work. Period.
But many people realize that we’re complex beings. It’s just not as simple as “just deal with it”. It’s not going to work to “just take a pill”.
And that brings us to one of the current “cool” terms in pain treatment, pain catastrophizing. (Say it out loud once or twice. It’s fun.)
Pain catastrophizing has been defined in various ways, but here’s the basic idea. Everyone seems to think differently about pain (and think differently at different times, in response to different types of pain, and so on). Some thoughts may be positive (“It will be over in a few hours”) and some thoughts may be negative (“There’s nothing I can do to make things better”).
If those thoughts are on a basically negative path, it can make things even worse than the pain would by itself. That’s pain catastrophizing.
I’ve often said that how you think about pain is directly related to disability. In other words, if I’m constantly thinking about my pain, I am more disabled. I may have more pain another day, but if I find a way to think about it less, it affects how disabled I am.
This may not mean that thoughts affect the pain – actually making it more or less. But it does affect – as I said – disability. It affects behaviour. It may change even the treatments I choose, or how productive I am, to some extent.
Because thoughts are so personal, and pain is so personal, this is a very slippery topic. Many researchers believe pain catastrophizing exists (let’s call it PC from now on in this article), but here are some of the big questions that we have.
What causes PC? Is it simply caused by too much pain too often? Or is it more a matter of culture, or point of view, or behaviour?
Can PC actually directly make symptoms worse? How?
Can PC actually be treated directly?
Do different types of pain change how PC works?
Various methods have been used to measure PC, or related things like your anxiety regarding your pain, or fear avoidance. For example, PC is measured using rumination, magnification and helplessness. Rumination is a focus on your symptoms, causes, and consequences (for example, continually thinking about the pain). Magnification is an exaggeration of your symptoms or circumstances (“what if I’m dying?”). Helplessness is – well, you can guess! Things like saying “there’s nothing I can do about these symptoms!”
But trying to measure responses to pain are difficult when someone else can’t really measure your pain. And how accurately do we even understand our thoughts over the past 24 hours?
Treating Pain Catastrophizing?
That’s the question, isn’t it? Can it be treated?
Some researchers thought, if it’s all about positive attitude, could an anti-depressant pill treat it? Results have been less than positive on that front.
No silver bullet has been found to “treat” PC. As Dr. Steven Z. George (associate professor of physical therapy at the University of Florida in Gainesville) put it,
Other studies have shown SSRIs [common antidepressants] not to be very effective or to be less effective. For now, the mainstay of treatment is cognitive-behavioral therapy (CBT). This may include learning better coping skills, and practicing acceptance and mindfulness. But we still have to treat the pain. It is a bit of the chicken and the egg. Which comes first? If we reduce that pain, catastrophizing gets better. If we reduce the catastrophizing, pain gets better. [source]
In other words, it’s just what we’ve been saying all along. You have to treat the whole, complex, human being. Positive thinking doesn’t generally make pain vanish (and would we want that? If you convince yourself you have no pain, you put yourself in serious danger of not listening to your body’s warning signals). But your thoughts do work together with your behaviour to make your treatment work.
It’s also tempting to rely on the power of placebo. “Who cares if xyz isn’t a treatment with any scientific evidence whatsoever? If you think it works for you, it does.” But – wouldn’t it be all the better if you “thought” that a treatment with good evidence behind it worked?
In the end, both doctors and patients need to be aware of PC. We need to stop ignoring the fact that our thoughts do make a big difference in our level of disability. No, that’s not the answer to all our problems. But it is a part of the complex picture.
If you’d like to learn more, check out these articles:

 Narcolepsy is actually quite a serious chronic sleep disorder. Basically, sleep can sneak up and attack you during the day – for example, you may be extremely drowsy during the day, you may end up with muscle weakness/slurred speech/loss of muscle control, and you may even experience hallucinations.
Narcolepsy is actually quite a serious chronic sleep disorder. Basically, sleep can sneak up and attack you during the day – for example, you may be extremely drowsy during the day, you may end up with muscle weakness/slurred speech/loss of muscle control, and you may even experience hallucinations.
 This is a helpful chart, but let me explain it. There are three sets of data. First, those who had a quarterly injection (before, and after, basically), then those who had a monthly injection, and then a placebo.
This is a helpful chart, but let me explain it. There are three sets of data. First, those who had a quarterly injection (before, and after, basically), then those who had a monthly injection, and then a placebo. Pain catastrophizing has been defined in various ways, but here’s the basic idea. Everyone seems to think differently about pain (and think differently at different times, in response to different types of pain, and so on). Some thoughts may be positive (“It will be over in a few hours”) and some thoughts may be negative (“There’s nothing I can do to make things better”).
Pain catastrophizing has been defined in various ways, but here’s the basic idea. Everyone seems to think differently about pain (and think differently at different times, in response to different types of pain, and so on). Some thoughts may be positive (“It will be over in a few hours”) and some thoughts may be negative (“There’s nothing I can do to make things better”).