A New Nasal Spray, and some Tips (podcast)
A new podcast from Headache and Migraine News – hope it’s a help to you!
Podcast: Play in new window | Download
Resources related to the podcast:

A new podcast from Headache and Migraine News – hope it’s a help to you!
Podcast: Play in new window | Download
Resources related to the podcast:
Treating migraine in the emergency room of a hospital is a challenge, and opinions and methods are changing rapidly. Narcotics were once common, but researchers began to discover that patients taking narcotics in emergency (instead of other treatments – more on that in a moment) actually tended to be in the hospital longer and come back more often. This isn’t to suggest that they were “drug seekers”, but simply that the narcotics were less effective than was once believed – and side effects were more common.

And older medication, dihydroergotamine, has been persistently used as well.
A meta study published this month in the American Journal of Emergency Medicine highlighted some of these changed (see link at bottom of this article). Comparing how things were at the turn of the millennium, the study found:
Narcotics are only give 1/3 as often as they were. Not only that, “discharge prescriptions” are down to a third or less or what they were.
An obvious question is – are the new procedures helping? That may be a complex question, but the same study did find that return-to-emergency rates were also down, to a third of what they were back in 1999-2000.
That return rate may not be quite as great as it sounds – only 12% returned before, now only 4%. Still, a significant difference.
For more on emergency room procedures, see:
Zecuity, the skin patch for migraine, has had a bad month.
On the 2nd of June (this month), the FDA announced that they are investigating the risk of burns from the patch:
The U.S. Food and Drug Administration (FDA) is investigating the risk of serious burns and potential permanent scarring with the use of Zecuity (sumatriptan iontophoretic transdermal system) patch for migraine headaches. We are investigating the cause and extent of these serious side effects and will update the public with new information when our review is complete.
FDA Drug Safety Communication
 On the 10th, Zecuity manufacturer Teva Pharmaceuticals decided to temporarily stop sales and marketing:
On the 10th, Zecuity manufacturer Teva Pharmaceuticals decided to temporarily stop sales and marketing:
Teva has been working closely with the FDA to examine reported adverse skin reactions associated with ZECUITY usage. At Teva, we are deeply committed to the safety and well-being of people who use our products. As such, we have decided to engage in a voluntary suspension of the sale, marketing, and distribution of ZECUITY while we continue our investigations into the root cause of these adverse skin reactions. In keeping with this market suspension, we have initiated a pharmacy-level recall of the product.
Letter from Teva
Patients are advised to stop using the Zecuity patch right away.
The symptoms some patients have reported include itching, burning, and other pain. Some of the skin reactions were not resolved after several months.
It’s not clear exactly what is causing these reactions. This is, of course, a well-tested product. It’s hard to speculate whether the product could actually return to the market as-is with further warnings/instructions, or if it will have to go back for further testing.
Zecuity is a method to take sumatriptan. If any medication can be taken in many ways, it’s sumatriptan. However, as we all know, there are those out there who have probably been helped by Zecuity who haven’t been helped by other treatments. (More on this product)
Another issue is that this technology holds great promise for other migraine treatments and beyond. It would be a shame if there was another major setback, although hopefully this will be an opportunity to further improve skin patch products.
Important to know:
Have you ever had to give yourself an injection? I have. Not fun.
That was the question in our most recent poll, and here are the results:
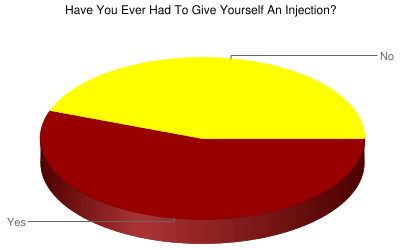 Over 55% of you said “yes”. And I’m sure many of those would be talking about multiple injections.
Over 55% of you said “yes”. And I’m sure many of those would be talking about multiple injections.
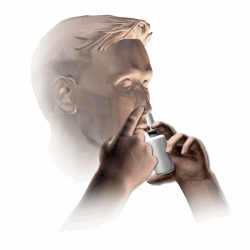
Taking medications via a needle is a common method to stop a migraine attack after it starts. Medications such as sumatriptan and dihydroergotamine may be injected to get the medication into your system faster.
The downside is that a migraine patient may be more sensitive to pain, and may be suffering from nausea, and using a needle may be a very big deal.
But medical technology is starting to give us other options. Some delivery systems may be almost as good – or as good – or even better than injections.
Take for example nasal sprays and nasal powders, needle free injection systems, and skin patches.
If you find injections helpful, but very difficult to do (due to the pain, or other reasons), talk with your doctor about some of the many options out there.
While you’re here, check out the right side bar of the website for the latest poll!
New research is confirming the benefits of a medication that can fight episodic migraine. It might be just the thing to try if you haven’t had success with the medications your doctor has prescribed up to this point.
Many migraine patients are familiar with Toradol, or ketorolac tromethamine. Ketorolac is actually one of the top recommended drugs to give a migraine patient in emergency. It’s low on side effects and high on effectiveness.
Today, ketorolac is available as a nasal spray – perfect for those trying to avoid injections but who still want something that’s fast-acting. The nasal spray is commonly sold under the brand name Sprix.
 But how does this medication compare to migraine-specific medications, such as the ever-popular sumatriptan?
But how does this medication compare to migraine-specific medications, such as the ever-popular sumatriptan?
A study in the journal Headache this past February attempted to answer the question, pitting ketorolac nasal spray against sumatriptan nasal spray.
In a double-blind study of 72 randomized participants were treated for 152 migraine attacks.
The results? Ketorolac was every bit as good as sumatriptan – in fact, in some ways it had the edge. The pain relief seemed to last longer, and ketorolac was better at fighting nausea. It also helped fight photophobia, that painful sensitivity to light that many migraine patients experience.
More good news – none of the patients, taking either of the two medications, withdrew from the study due to side effects.
These things make a nasal spray such as Sprix very attractive for those with episodic migraine.
However, ketorolac is not recommended for chronic migraine. It is intended for very occasional use. There are cardiovascular and gostrointestinal risks if the medication is taken frequently, or if it’s taken constantly for more than a few days (read more here). For migraine patients who already may be at increased risk in these areas, frequent use of ketorolac should be avoided.
But those with episodic, or more occasional, migraine still face another hurdle. This medication can be very expensive. However, Dr. Alexander Mauskop from the New York Headache Clinic has an excellent suggestion to save money. He writes:
The main problem with intranasal ketorolac is its cost. On GoodRx.com the price of 5 vials of Sprix (with a coupon) is about $1,000. Each vial is good for one day of use; it contains 8 sprays (15 mg each) and the usual dose is one spray into each nostril, repeated every 6 hours as needed. However, there is a way around the cost of this medication. Ten 30 mg vials of generic ketorolac for injections cost $15. You just need to buy a nasal spray bottle, empty the contents of the vial into it and use it as needed.
Check with your doctor and your insurance company to confirm which option is best for you.
To read the ketorolac vs. sumatriptan study results, visit A Randomized Trial of Ketorolac vs Sumatripan vs Placebo Nasal Spray (KSPN) for Acute Migraine
.jpg){kind=link}